Best Hospital Management System for Multi-Speciality Hospitals (50–500+ Beds)
A **Hospital Management System (HMS)** for Indian multi-speciality hospitals (50–500+ beds) is an integrated software platform that digitizes medical records and clinical operations across OPD, IPD, OT, LIS, and billing departments. Cliniqwise provides a secure, flat-fee HMS that cuts patient registration wait times to under 10 seconds via ABDM ABHA QR codes, handles cashless claims via the government's NHCX claims integration portal, and keeps clinical data compliant under the Digital Personal Data Protection (DPDP) Act 2023, with full onboarding completed within 14 days.
Most multi-speciality hospitals experience revenue loss because legacy systems cannot organize departmental workflows: managing multiple doctor schedules, ward billing, inter-departmental transfers, and corporate insurance claims. A proper implementation takes 8 to 12 weeks for a 100–200 bed hospital, requiring a phased approach to prevent system disruptions.
This evaluation guide compares leading hospital management software solutions—MocDoc (module-based SaaS), CrelioHealth (lab-focused diagnostic HIS), and Cliniqwise (fixed flat subscription with WhatsApp integration)—helping directors, medical superintendents, and IT managers select the ideal platform.
Quick Answer: How to Choose a Multi-Speciality HMS
For a 50–500+ bed multi-speciality hospital in India, your software must check these three boxes:
- •Covers all departments: OPD schedules, bed transfers, OT slots, central pharmacy stock, and lab report tracking on one database.
- •India-ready compliance: ABHA creation & health locker sync (ABDM), direct digital cashless insurance (NHCX), NABH guidelines, and secure data handling (DPDP Act).
- •Clear cost mapping: Predictable pricing models that include support, data transfers, barcode printers, and clinician training.
Comparing Key Vendors:
Your final choice depends on your patient volume, bed size, internet stability, and how fast your nursing staff and senior consultants can learn the new system.
Why Multi-Speciality Facilities Need Custom Features
Running a multi-speciality hospital is much more complex than managing a single OPD clinic. Multiple departments share resources, bed availability changes hourly, and billing requires sync between doctors, labs, and ward charges.
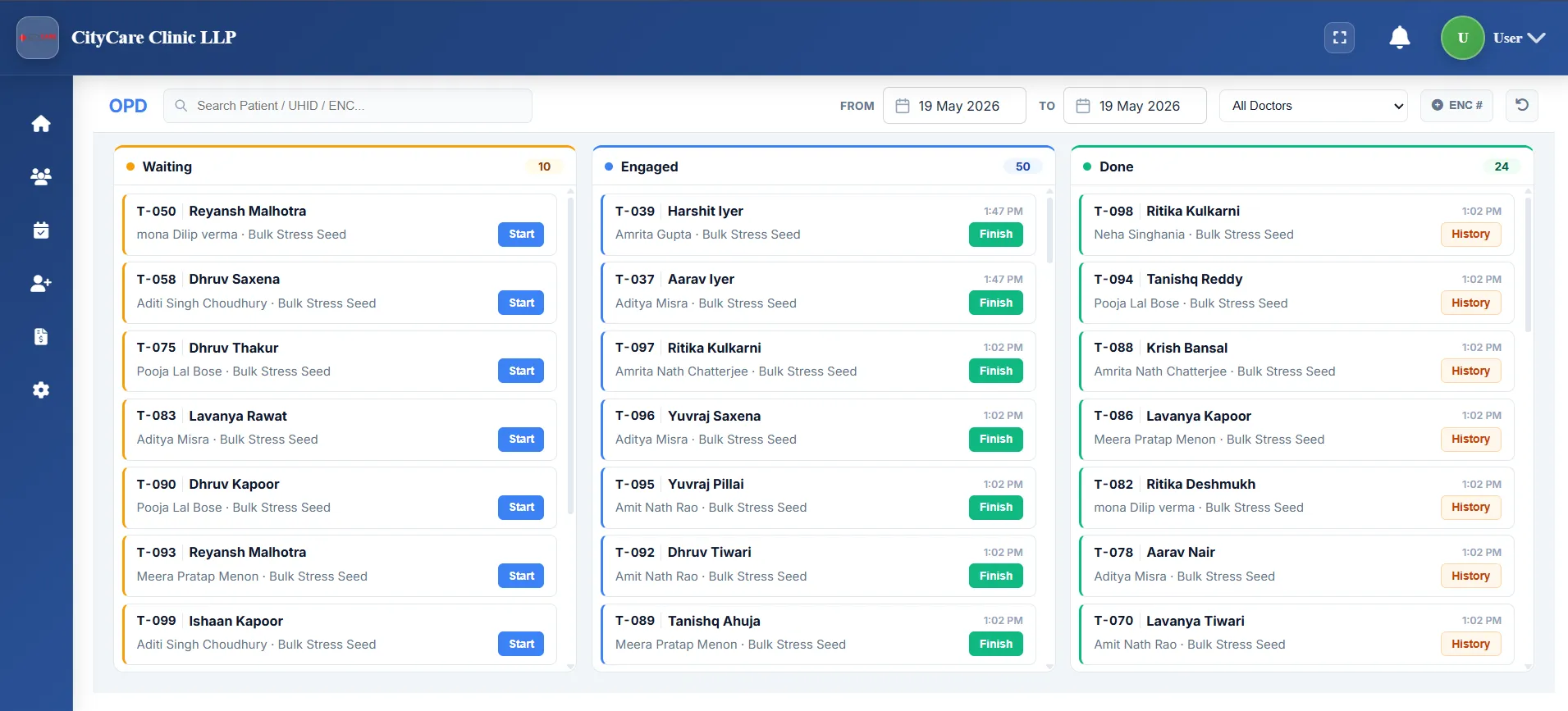
OPD Management - Multi-Department Flow
Organizes appointment lists across Orthopedics, Pediatrics, Gynecology, General Medicine, and Surgery, assigning doctor schedules and patient routing.
Core Needs: Fast patient registration, queue screens, emergency walk-ins, and direct sharing of files between consulting doctors.
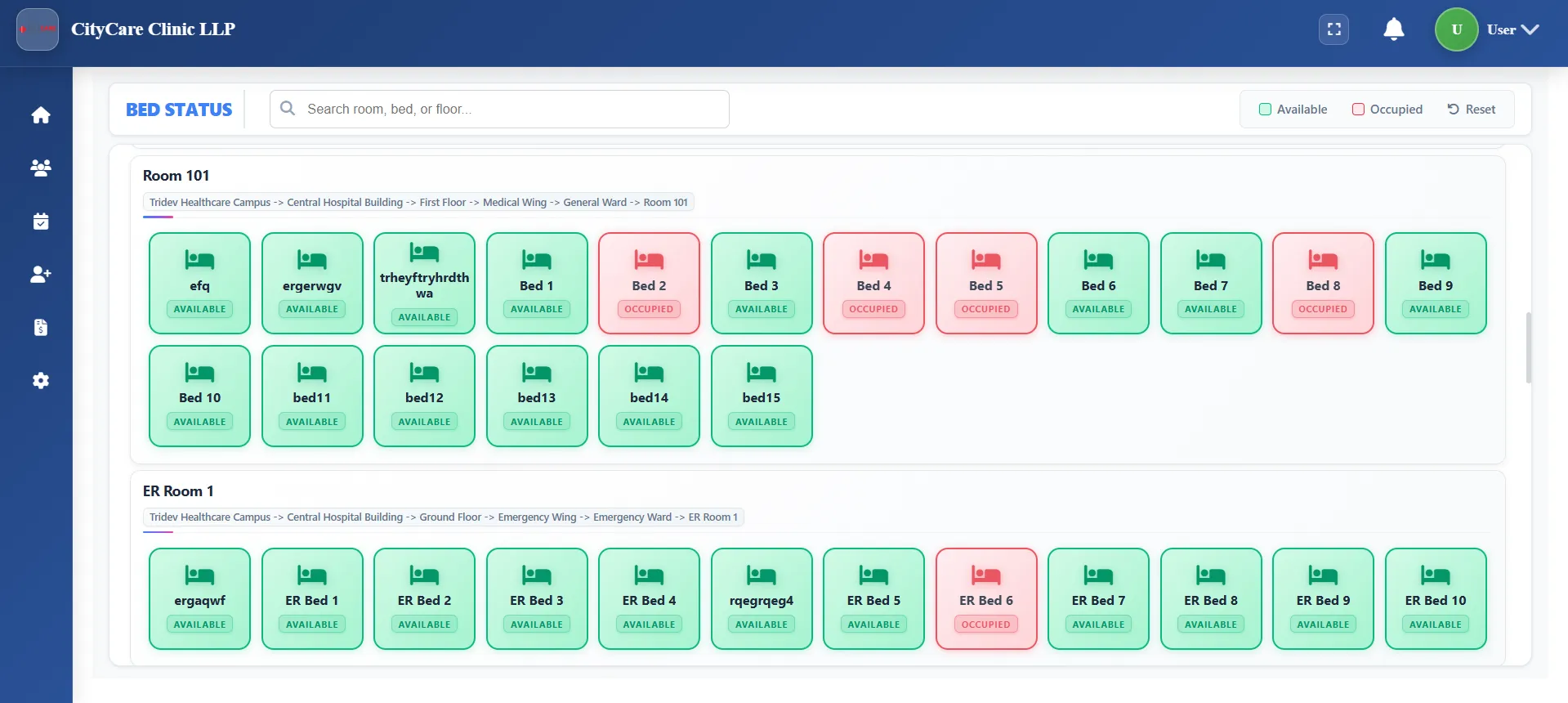
Ward & Bed Allocations (Admission-Discharge)
Tracks occupied beds, active patient admissions, and ward transfers across ICUs and private rooms.
Core Needs: Nurses and doctors must see the same digital map showing who is occupied, pending discharge, or transferring.
OT Bookings & Post-Op Notes
Schedules surgeries across Operation Theatres, assigning surgeon schedules and logging post-op clinical notes.
Core Needs: Surgical notes template, anesthesia logs, and automatic transfer of drug use details to ward billing.
Pharmacy, Lab, & Billing Counter Sync
Syncs pharmacy stock updates, lab machine data, radiology files, and bill approvals.
Core Needs: Direct machine sync to save staff time, automated lab reports, and claims preparation using the standard NHCX network.
India Digital Health Stack – ABDM, NHCX, NABH, & DPDP
Medical software in India must align with government guidelines. Selecting an outdated system can lead to problems with cashless insurance approvals and compliance audits.
ABDM M1, M2, M3 Milestones
The Ayushman Bharat Digital Mission (ABDM) has three active phases for software:
- M1 (ABHA IDs): Creating and verifying patient ABHA cards, and registering doctors in central registries.
- M2 (Linking Health Records): Linking OPD prescriptions, lab findings, and discharge summaries to patient ABHA profiles.
- M3 (Digital Consent Sharing): Enabling patients to share records with other hospitals securely using standard consent APIs.
NHCX – Cashless Claims Exchange
The official National Health Claims Exchange (NHCX) standardizes insurance data sharing between hospitals, private TPAs, and public health schemes.
An NHCX-ready HMS handles:
- • Creating standard digital claim documents.
- • Sending claim updates to multiple insurance providers through one protocol.
- • Checking data fields for errors before submission to lower claim rejection rates.
NABH Guidelines for Medical Records
The NABH standards require strict controls over how medical records are created, updated, and stored.
The software must maintain complete change logs (audit trails), handle user access levels securely, and follow standard templates for clinical notes.
Key features to check:
- • Easy retrieval of medical records during audits.
- • Standardized formats for nursing charts and drug administration records.
DPDP Act 2023 – Patient Data Security
The Digital Personal Data Protection (DPDP) Act 2023 requires hospitals to protect patient information, obtain clear consent, and prevent unauthorized data sharing.
Key requirements for your IT setup:
- • Clear mechanisms to allow patients to request data deletion or correction.
- • Strict user permission levels, secure data storage, and detailed access tracking.
- • Tracking and storing patient consent before sending promotional alerts.
HMS Evaluation Checklist
Use these four categories to evaluate software vendors during their product demonstrations.
Clinical Usability
- • Specialty templates for different doctors?
- • Quick internal referrals between OPDs?
- • Nurse records and vitals sync?
Ease of Learning
- • Minimum clicks for writing a prescription?
- • Tablet-friendly interface?
- • Main workflows grouped on 1-2 pages?
Tech Integrations
- • Cloud server uptime guarantee and backups?
- • Direct lab machine data extraction?
- • User login security levels?
Support & Setup
- • Support through account managers or ticket queues?
- • Expected setup timeline?
- • Reference clients with similar bed counts?
Feature Priorities by Bed Size
The software requirements change based on the size and complexity of your facility.
| Bed Count | Facility Type | Priority Modules | Key Risk Factor |
|---|---|---|---|
| 50–99 beds | Single location; 2-3 OTs, general ICU. | Quick setup, main OPD/IPD bill formats, pharmacy, basic lab sync. | Overpaying for high-end features your team won't use. |
| 100–199 beds | Multi-speciality setup; active insurance caseload. | Detailed ward maps, OT schedules, LIS sync, insurance paperwork (TPA), ABDM integration. | Using multiple disconnected systems, causing manual entry errors. |
| 200–349 beds | Regional referral hospital with secondary centers. | Cloud speed, management dashboards, NHCX claims, multi-center sync, high data safety. | System lag, expensive customized update requests from vendors. |
| 350–500+ beds | Flagship group with multiple campuses. | Enterprise databases, full API integrations, custom development, strict security settings. | Complicated staff training, high software subscription costs. |
HMS Pricing Models and Hidden Costs
Standard cloud hospital systems typically charge per user or doctor. However, the base subscription quote often does not cover additional setup charges.
| Pricing Model | How It Works | Advantages | Drawbacks | Best Fit For |
|---|---|---|---|---|
| Per-user / per-doctor SaaS | Monthly charge per doctor/billing user | Low initial cost to launch | Pricing grows quickly as you hire consultants and ward staff | Outpatient clinics and small doctor networks |
| Per-module licensing | Base software fee + extra fees for LIS, OT, Pharmacy, etc. | Only pay for the modules you implement | Adding extra departments later can be expensive | Hospitals rolling out digital tools in slow phases |
| Flat subscription (hospital-wide) | One fixed subscription for the whole hospital based on beds | Predictable yearly budget, unlimited users/doctors | Slightly higher entry cost compared to basic tools | Facilities looking for flat costs and deep team adoption (Cliniqwise) |
| On-premise license | One-time license purchase + annual maintenance (AMC) | Total control of database on local hardware | Requires in-house IT staff, expensive servers, manual updates | Large groups with dedicated server rooms and strict policies |
Cost Breakdown Checklist
Make sure to budget for these operational expenses:
- • Wi-Fi & LAN setup: CAT6 cables, managed access points, and backup UPS for systems.
- • Barcode printer hardware: Sticker machines, scanners for pharmacy counters, and sample tubes.
- • Ward devices: Android tablets for nurses and consultants doing ward visits.
- • Implementation support: Transferring active patient files and training staff.
- • Compliance checks: Safety tests required to meet patient data regulations (DPDP Act).
Cliniqwise Cost Structure
To prevent unexpected price rises as you add consultants, rooms, or departments, Cliniqwise uses a **flat subscription model**.
You do not pay per doctor account, per invoice generated, or per appointment. This keeps your yearly software expenditure completely predictable.
Pricing and Cost Matrix
Ask vendors these questions to avoid hidden fees in your service agreements.
| Item | Type | Questions to Ask | Things to Avoid |
|---|---|---|---|
| Software License | Recurring Subscription | Are all modules (IPD, Pharmacy, LIS) included? Are there limits on doctor accounts? | Limits on doctor profiles or active bed updates that trigger extra fees. |
| Setup & Training | One-time | How many training days are included? Is there support during the launch week? | Extra billing for training new staff hires or retraining. |
| Hardware Sync | One-time | Is the software compatible with standard barcode printers and lab machines? | Being forced to buy specific, expensive printer brands from the vendor. |
| Data Transfer | One-time | Can you migrate our active patient list and drug stocks from our old software? | Hidden fees for data conversion or long timelines. |
| Compliance Updates | Included/Recurring | Are future changes for ABDM and NHCX included in the base price? | Paying for mandatory updates whenever government rules change. |
MocDoc vs CrelioHealth vs Cliniqwise
A direct comparison of features, pricing structures, and implementation support.
| Details | MocDoc | CrelioHealth | Cliniqwise |
|---|---|---|---|
| Focus Area | Integrated HMS with modules for OPD/IPD billing, pharmacy stock, and lab operations. | Lab system (LIS) and diagnostic features. Very strong machine integrations. | Full hospital system with bed maps, touch-friendly screens, and direct doctor prescription flows. |
| Best Suited For | Medium hospitals looking for standard cloud billing and inventory tools. | Standalone diagnostic chains or lab-heavy hospitals. | Hospitals prioritizing quick staff adoption, flat costs, and patient alerts on WhatsApp. |
| Pricing Structure | SaaS rates based on setup size and modules used. | SaaS rates, often based on lab test counts or branches. | Flat yearly subscription based on bed brackets. No per-doctor surcharges. |
| Prescription Flow | Web forms. Detailed but can require multiple pages. | Basic patient record views; optimized for lab output. | Simple one-screen prescription writer, designed to help doctors wrap up visits quickly. |
| WhatsApp Sync | SMS alerts; WhatsApp features vary by plan. | Strong result distribution for lab patients. | Sends prescriptions, billing updates, and lab reports directly to the patient's WhatsApp. |
| Setup & Support | Support via standard call support and email tickets. | Standard software setup guides. | Dedicated setup support manager with agreed SLA response times. |
Key Strengths of Cliniqwise for Multi-Speciality Setups
How we help hospital owners streamline administration and keep software overhead predictable.
Predictable Subscription
A flat-rate subscription that stays the same even as you add new doctors, specialists, or billing desks.
One-Screen Clinical Note
Prescriptions, diagnostic orders, and diagnoses are entered on a single page, reducing typing work for senior consultants.
WhatsApp-First Alerts
Delivers bills, e-prescriptions, and laboratory findings straight to the patient's WhatsApp number in digital PDF format.
Ward & Bed Boards
ADT, room assignments, OT logs, and pharmacy stocks are managed through touch-screen layouts for nursing staff.
Direct Support Team
A named account manager handles your setup, updates, and compliance audits instead of anonymous chat widgets.
Launch & Staff Training Timelines
A typical cloud HMS setup takes 8 to 12 weeks to complete staff training and patient list migration. For larger facilities, we recommend a phased approach.
Phase 1: Pricing & Forms (Weeks 1-3)
Configuring OPD doctor schedules, uploading drug lists, and saving standard bill settings.
Phase 2: Department Training (Weeks 4-6)
Activating front-desk billing, central pharmacy counters, and training lab techs and ward nurses.
Phase 3: Parallel Launch (Weeks 7-10)
Running the new software alongside old registers for 2-3 weeks to verify numbers before complete switchover.
Best Practices for a Smooth Launch
- 1. Phase 1 RestrictionsAvoid requesting custom program changes during Phase 1. Focus on standard features first.
- 2. Department Super-UsersPick one lead doctor, nurse, and biller to act as setup champions for their teams.
- 3. Launch Parallel TestingRun active checks between billing logs in the old and new systems during the parallel phase.
What Indian Hospital Directors Say
“Cliniqwise implemented ABDM & NHCX inside our hospital in under 2 weeks. Our billing leakage stopped completely and we're now 100% compliant.”
Dr. Amit Khandelwal
Chief Medical Director, Apple Hospital
“Our OPD wait times reduced from 45 minutes to less than 10 minutes using the ABHA Scan & Share token system. Incredible product!”
Dr. S. K. Singh
Senior Consultant & Director, Bundelkhand Hospital
“The automatic doctor commission tracking and ward billing saved our finance team 40+ hours every single month. Highly recommended for busy facilities.”
Dr. R. K. Choudhary
Managing Director, Krishna Hospital
Frequently Asked Questions
How long does it realistically take to implement an HMS in a 100–200 bed multi-speciality hospital?
If infrastructure (network, devices) is ready, cloud HMS platforms can be configured in a few weeks, but realistic go-live timelines for a 100–200 bed multi-speciality hospital, including training, data migration, and a parallel run, are usually 8–12 weeks. Larger hospitals or those with heavy customisation and integrations (LIS/RIS, NHCX, ERP) should plan for staged go-lives over 3–6 months.
How should we handle offline or low-connectivity situations?
For hospitals with unstable connectivity, prioritise an HMS that caches key screens and allows temporary offline capture of notes and orders, then syncs when the network is back. It should keep the core database on a reliable central server (cloud or on-prem) but use local Wi-Fi for ward/OPD access, and offer clear downtime procedures aligned with NABH information management guidelines.
What is the safest way to migrate from a legacy HMS or partial EMR?
Safe migration involves identifying what must move (patient master, active IPD cases, recent OPD history, billing balances) versus what can be archived in read-only form, running dual systems for a short period while validating consistency, and ensuring both systems are available in parallel during audits. Avoid mass free-text imports without structure.
How do ABDM and NHCX practically affect my hospital’s software choices?
ABDM compliance standardises patient identity via ABHA and enables electronic health record sharing under patient consent. NHCX standardises and digitises health insurance claims, cutting cashless claim rejection rates and accelerating payout cycles. Choosing an HMS that supports ABDM M1-M3 and is NHCX-ready reduces future integration costs.
How does the DPDP Act change what I should demand from my HMS vendor?
Under the DPDP Act 2023, hospitals must obtain explicit, informed consent for data processing, implement strong security controls, give patients access/correction rights, and notify authorities of breaches. Your HMS must offer granular consent logs, role-based access, encryption, robust audit trails, and data erasure tools.
How can we minimise resistance from senior consultants and nursing staff when rolling out a new HMS?
Involve clinical leaders early in template design, choose systems with low-click, single-screen consultation flows, and provide tablet-friendly interfaces. Offer short, role-specific training sessions, place super-user champions in each ward, and ensure highly responsive, relationship-centric support via named managers.
Official Regulatory Resources & Citations
Ready to choose an HMS your team will actually adopt?
Book a detailed implementation roadmap audit for your multi-speciality hospital. Let us show you a low-click EMR workflow, ABDM-linked charts, and automated billing in action.